

Introduction
Healthcare organizations face two compounding pressures: escalating cyberattacks and mounting regulatory scrutiny. For the 14th consecutive year, healthcare reported the most expensive data breaches across all industries, averaging $7.42 million per incident in 2025.
The sector is a persistent target for a straightforward reason: protected health information (PHI) commands premium prices on dark web markets, and many healthcare systems still run legacy infrastructure vulnerable to well-documented exploits.
Most healthcare security incidents trace back to preventable vulnerabilities. The 2025 Verizon Data Breach Investigations Report documented a 180% increase in vulnerability exploitation as the primary breach entry point. A structured vulnerability management program closes these gaps systematically - before regulators issue fines or attackers find their way in.
Overview
- Healthcare faces disproportionate cyber exposure due to legacy systems, connected medical devices, and complex third-party dependencies
- Unmanaged vulnerabilities trigger HIPAA violations, ransomware outages, and patient safety risks - with breaches averaging $7.42 million
- Effective programs cover five steps: asset discovery, continuous scanning, risk-based prioritization, systematic remediation, and audit documentation
- Patch backlogs beyond 90 days, missing asset inventories, and infrequent scanning are red flags that signal a program in trouble
- Ongoing protection depends on continuous monitoring, staff training, and documented policies updated regularly
Common Sources of Healthcare Security Vulnerabilities
A security vulnerability in healthcare is any weakness in a system, process, or control that could allow unauthorized access to electronic protected health information (ePHI) or disrupt clinical operations. Healthcare environments face a disproportionate concentration of these weaknesses compared to other industries due to aging infrastructure, operational complexity, and the sheer volume of connected devices.
Healthcare vulnerabilities typically arise from a combination of technical debt, operational constraints, and organizational gaps - not a single root cause. Each category requires a different response.
Legacy Systems and Unpatched Software
Many hospitals and clinics continue running outdated operating systems, legacy EHR platforms, and medical devices that no longer receive vendor security updates. Research shows that 14% of connected medical devices run on unsupported or end-of-life operating systems, making them attractive targets for exploits that have known patches elsewhere.
IT teams routinely defer upgrades to avoid disrupting clinical workflows - creating a growing backlog that attackers actively scan for. The scale of the problem is hard to ignore:
- 44% of healthcare organizations operate devices with known, unpatched vulnerabilities
- 28% run devices past their end-of-support dates
- Unpatched legacy systems consistently rank among the top initial access vectors in healthcare ransomware incidents
Shadow IT and Untracked Assets
Healthcare departments often deploy their own cloud applications, connected devices, and test environments without IT oversight. These "shadow" assets are rarely scanned or patched and represent invisible entry points for attackers.
The rapid adoption of Internet of Medical Things (IoMT) devices, telehealth platforms, and AI-powered diagnostic tools has significantly expanded the healthcare attack surface. Smart hospitals worldwide are projected to deploy 7.4 million connected IoMT devices by 2026, averaging over 3,850 devices per hospital. Yet 60% of health systems report an inability to adequately protect unpatchable or agentless medical devices, and 56% cite poor device visibility as a major limitation.

Weak Access Controls and Insider Risks
Excessive user privileges, shared credentials, and inadequate multi-factor authentication create vulnerability conditions that external attackers and inadvertent insiders exploit equally. In healthcare "Basic Web Application Attacks," 88% of breaches involve the use of stolen credentials.
Once a staff credential is compromised, attackers gain lateral movement access across systems storing PHI - often going undetected for weeks. The median dwell time in non-actor-disclosed breaches is 24 days, which is enough time to exfiltrate sensitive records or stage a ransomware deployment.
Third-Party Vendor and Business Associate Exposure
Healthcare organizations share PHI with dozens of vendors - billing platforms, labs, insurers, and cloud providers. The average modern hospital relies on more than 1,300 external vendors, each a potential weak link without verified, monitored security controls.
HIPAA's Business Associate Agreement (BAA) requirements create a compliance obligation, but signing a BAA doesn't guarantee a vendor's technical controls are sufficient. Business associates accounted for only 21% of breach reports to OCR in 2023 - yet those breaches affected 49% of all impacted individuals, over 55 million people.
What Happens When Healthcare Vulnerabilities Go Unmanaged
HIPAA's Security Rule requires covered entities to implement reasonable and appropriate safeguards. Documented vulnerability management failures are among the most common findings in HHS Office for Civil Rights (OCR) investigations, carrying civil penalties that can reach millions of dollars per violation category.
A concrete example: In 2024, Heritage Valley Health System agreed to a $950,000 settlement and corrective action plan following a ransomware attack. OCR's investigation found the system failed to conduct an accurate and thorough risk analysis of potential risks and vulnerabilities to ePHI, as required by 45 C.F.R. § 164.308(a)(1)(ii)(A).
Operational consequences extend beyond fines. Ransomware attacks targeting unpatched healthcare systems have forced hospitals to divert patients, cancel surgeries, and revert to paper records. The mean cost for healthcare organizations to recover from a ransomware attack was $2.57 million in 2024.
The May 2024 attack on Ascension health system illustrates the stakes: facilities diverted emergency patients, postponed procedures, and reverted to paper charting for weeks while systems were restored.
The reputational and patient safety dimension is direct and measurable. A PHI breach erodes patient trust, and the downstream care risks - unavailable imaging, inaccessible medication records - can affect patient outcomes before the breach is even contained.
Warning Signs You're About to Experience a Security Incident
These operational red flags often precede breaches - not hypothetical risks, but observable conditions security teams can audit today:
- Scans are infrequent or unauthenticated - running less than monthly, or unable to log into systems to verify patch levels, leaving large exposure windows between cycles
- No documented asset inventory - the organization can't quickly list all servers, endpoints, medical devices, and cloud workloads, meaning unknown assets go unmonitored and unpatched
- Patch backlogs exceeding 90 days - critical or high-severity vulnerabilities remain open past remediation SLAs with no documented exception or compensating control, a pattern regulators treat as evidence of inadequate risk management
How to Reduce HIPAA Security Risks Through Vulnerability Management
Vulnerability management is not a one-time project but a continuous cycle aligned with HIPAA's requirement for ongoing risk analysis and risk management under 45 CFR §164.308(a)(1). The five-step framework below provides a systematic approach to closing security gaps before they become breach headlines.
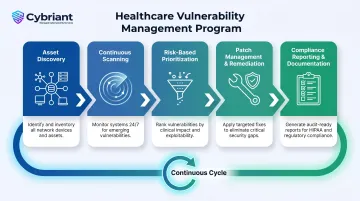
Step 1 - Asset Discovery and Inventory
Build and maintain a real-time inventory of all IT assets - servers, workstations, cloud resources, applications, and biomedical/IoMT devices - using automated discovery tools and DHCP/NAC logs.
Why this matters: You cannot protect what you cannot see. An accurate inventory ensures every asset is in scope for scanning, patching, and access control reviews, eliminating the blind spots attackers exploit. Without this foundation, vulnerability management programs fail before they begin.
Asset discovery should run continuously, with automated alerts triggered when new devices connect to the network. Quarterly manual reconciliation helps catch gaps automated tools might miss.
Step 2 - Continuous Vulnerability Scanning
Deploy authenticated vulnerability scanners that log into systems to verify actual patch levels. This approach should cover cloud and hybrid environments as well as medical device networks, using vendor-approved scan profiles that won't disrupt sensitive equipment.
Authenticated scanning surfaces a significantly larger share of real vulnerabilities than unauthenticated scans - particularly in patient portals, EHR systems, and APIs where PHI flows. Unauthenticated scans probe the perimeter without credentials, missing vulnerabilities tied to installed packages or native services.
Scan general systems at least monthly and internet-facing assets weekly. Trigger additional scans after major changes or high-profile vulnerability disclosures. For healthcare organizations without dedicated security staff, Cybriant's real-time vulnerability scanning continuously monitors assets without requiring internal teams to manage scan schedules or interpret results.
Step 3 - Risk-Based Prioritization
Score vulnerabilities using four factors:
- CVSS severity as a baseline rating
- Exploitability in the wild - cross-reference CISA's Known Exploited Vulnerabilities catalog
- Asset exposure - internet-facing systems carry higher risk than internal ones
- Clinical criticality - does the affected system directly impact patient care?
This approach stops teams from burning time on low-risk findings while critical EHR or life-safety device vulnerabilities wait. Prioritize immediately after each scan cycle, using SLAs by risk tier:
- Critical: 7 days
- High: 30 days
- Medium/Low: 60–90 days
Step 4 - Patch Management and Remediation
Establish a formal patch management policy that defines:
- Roles and testing requirements
- Deployment schedules aligned with clinical maintenance windows
- Documented compensating controls - network segmentation, virtual patching, enhanced logging - for systems that can't be patched immediately
Structured remediation closes the exploitable window before attackers can act. The urgency is real: in 2024, organizations fully remediated only about 54% of edge device vulnerabilities, with a median remediation time of 32 days. Healthcare specifically averaged 71 days to remediate critical vulnerabilities - far longer than telecommunications at 12 days.
Patch management runs continuously. Apply emergency patches for actively exploited vulnerabilities within 24–72 hours. Healthcare organizations without a dedicated security team can partner with a managed provider like Cybriant - combining real-time scanning with automated patch management - to keep remediation on schedule without straining internal IT.
Step 5 - Compliance Reporting and Documentation
Generate audit-ready reports that map scan results, remediation actions, and exception approvals to HIPAA Security Rule requirements and recognized frameworks such as NIST CSF and HICP. Document not just what was found, but what was done about it.
This paper trail shows OCR auditors a clear record of active risk management and reduces penalty exposure if a breach occurs. The OCR's 2016–2017 HIPAA Audits Industry Report found that most covered entities failed to implement Security Rule requirements for risk analysis and risk management - and that poor documentation was among the most common findings.
Keep reporting ongoing: monthly operational dashboards for IT and security teams, and quarterly executive summaries tracking risk posture trends over time.
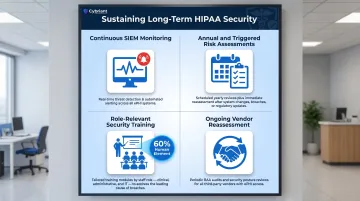
Long-Term Strategies for Sustained HIPAA Security
Vulnerability management is not a one-time project but a continuous discipline. Organizations that treat it as such significantly reduce breach probability and their exposure during HIPAA audits. Sustaining a mature program means weaving vulnerability management into daily security operations and staff habits.
Four practices form the backbone of any long-term HIPAA security program:
- Continuous SIEM monitoring: Feed vulnerability data and endpoint telemetry into a centralized SIEM to correlate events, detect anomalous behavior near ePHI, and speed up incident response. Organizations without 24/7 internal capacity can use a managed SIEM service - Cybriant's, for example, provides live monitoring around the clock without requiring a large in-house team.
- Annual and triggered risk assessments: Run a formal HIPAA risk analysis at least once a year and after significant changes - new systems, mergers, or new vendors - not just as a compliance checkbox, but as a real re-evaluation of your highest-risk areas.
- Role-relevant security training: Human error and phishing remain leading causes of healthcare breaches. 60% of breaches involve the human element, and 35% of healthcare organizations cite employees not following policies as the top cause of data loss. All clinical and administrative staff need regular, targeted training - not a once-a-year checkbox exercise.
- Ongoing vendor reassessment: Review business associates' security posture periodically - not just at onboarding. Request evidence of their vulnerability management practices and scan results where contracts allow.
Conclusion
Healthcare vulnerabilities have identifiable causes - legacy systems, shadow IT, access control gaps, and third-party dependencies - and each one is addressable with the right combination of process, tooling, and organizational commitment. The difference between organizations that experience preventable breaches and those that maintain strong security postures comes down to systematic execution of vulnerability management fundamentals.
A proactive vulnerability management program accomplishes three things simultaneously:
- Keeps your organization on the right side of HIPAA's Security Rule requirements
- Protects patient data before attackers find an exploitable gap
- Limits the operational and financial fallout that follows a preventable breach
Continuous scanning, risk-based prioritization, and timely remediation are not one-time projects - they're ongoing disciplines. Organizations that treat them that way build security postures that hold up under real-world pressure. Cybriant's managed vulnerability management services are built around exactly this model, giving healthcare organizations continuous visibility and faster remediation without the overhead of building that capability in-house.
Frequently Asked Questions
What are the 5 steps of vulnerability management?
The five steps are: discover (asset inventory), assess (vulnerability scanning), prioritize (risk-based triage), remediate (patching and compensating controls), and report (compliance documentation). In healthcare, this cycle must run continuously - not periodically - to keep pace with evolving threats and HIPAA requirements.
What is vulnerability in healthcare?
A healthcare security vulnerability is any weakness in a system, process, or control that could allow unauthorized access to PHI or disrupt clinical operations. Healthcare environments tend to carry more of these weaknesses than other industries due to legacy systems, connected medical devices, and third-party relationships that expand the attack surface.
What are the top 5 cybersecurity threats in healthcare?
The HHS Health Industry Cybersecurity Practices identifies ransomware, phishing and credential theft, unpatched legacy system exploits, third-party vendor breaches, and insider threats as the top risks. Most of these exploit vulnerabilities that a structured vulnerability management program is designed to address systematically.
What are 5 of the signs you should look out for when assessing vulnerability?
Key warning signs include infrequent or unauthenticated scanning, no maintained asset inventory, patch backlogs exceeding SLA thresholds, lack of formal vulnerability policies, and undocumented third-party access. These observable conditions are common precursors to HIPAA enforcement actions and successful breaches.
What is the biggest technology challenge facing healthcare today?
The combination of legacy infrastructure modernization and an expanding attack surface - IoMT devices, cloud services, APIs - represents the central technology challenge. This creates a vulnerability management burden that strains internal security teams, which is why many healthcare organizations turn to managed security providers to close the gap.
What are the 4 types of vulnerabilities?
The four categories are:
- Network vulnerabilities - unpatched systems, misconfigured firewalls
- Application vulnerabilities - software bugs, insecure APIs
- Physical vulnerabilities - unauthorized device access
- Human/process vulnerabilities - weak credentials, missing policies
Healthcare organizations typically face all four at once, which is why a siloed approach to remediation rarely works.


