

Introduction
Healthcare data breaches are not IT events that can be quietly resolved - they threaten patient safety, trigger regulatory enforcement, and cost organizations millions in recovery. The average healthcare breach now costs $7.42 million, the highest of any industry, with identification and containment taking an average of 279 days according to IBM's 2025 Cost of a Data Breach Report. Delayed procedures, EHR downtime, and disrupted medical devices translate into direct patient harm.
Despite widespread reference to incident response in compliance discussions, most healthcare organizations struggle to operationalize it. IR is a structured, cross-functional process designed to detect, contain, and recover from breaches while meeting HIPAA breach notification deadlines and preserving forensic evidence.
This article explains what healthcare incident response is, why it operates differently than in other industries, and how to execute it correctly - from initial detection through regulatory notification and full recovery.
Overview
- Healthcare incident response covers detection, containment, and recovery while meeting HIPAA notification deadlines
- Unique risks include patient safety exposure from downtime, PHI obligations, and medical device vulnerabilities
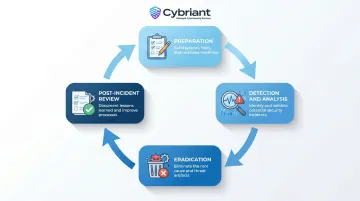
- The NIST SP 800-61 framework defines six IR phases: Preparation, Detection, Containment, Eradication, Recovery, and Post-Incident Review
- An untested plan isn't readiness - tabletop exercises, cross-functional teams, and evidence preservation all matter
- Formal IR plans paired with AI-powered security tools cut breach costs by up to $1.9 million and shorten breach lifecycles by over 100 days
What Is Healthcare Incident Response?
Healthcare incident response (IR) is the formal set of policies, procedures, and technologies an organization uses to identify, contain, and recover from cybersecurity incidents - particularly those involving protected health information (PHI) - while meeting HIPAA breach notification requirements.
Unlike general enterprise IR, it carries obligations that extend beyond operations: preserving forensic evidence, notifying regulators within mandated timeframes, and protecting continuity of patient care.
Three regulatory and clinical realities set healthcare IR apart:
- PHI breach presumption: HIPAA requires covered entities to assume a breach occurred unless they can prove otherwise through a documented risk assessment
- Mandatory HHS OCR reporting: Breaches affecting 500 or more individuals must be reported to HHS within 60 days
- Patient safety dimension: System downtime is not just an operational concern - it directly impacts clinical care, making containment decisions life-or-death choices
Done well, healthcare IR compresses detection-to-containment time, reduces breach costs, and keeps clinical systems available when patients depend on them most.
Why Healthcare Demands a Dedicated Incident Response Strategy
Healthcare remains the most targeted sector for cyberattacks. The 2025 Verizon Data Breach Investigations Report analyzed 1,710 incidents in healthcare, resulting in 1,542 confirmed breaches. System intrusions - including ransomware - now surpass miscellaneous errors as the top cause of healthcare breaches.
Patient Safety Stakes
Healthcare cyberattacks disrupt clinical operations in ways that directly harm patients:
- NHS WannaCry (2017): Resulted in a 6% decrease in total admissions at infected hospitals, 13,500 cancelled outpatient appointments, and 5 hospitals forced to divert emergency care
- Universal Health Services (2020): Staff resorted to pen and paper, facilities redirected ambulances, and the total financial impact reached $67 million
- Change Healthcare (2024): Disrupted healthcare operations nationwide, endangering patients' access to care
Each incident confirms that healthcare IR failures carry consequences far beyond stolen data - they delay diagnoses, divert ambulances, and put lives at risk.
HIPAA-Specific Obligations
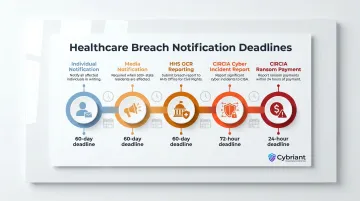
Healthcare IR plans must embed strict regulatory deadlines:
- Individual notification: Covered entities must notify affected individuals within 60 days of discovering a breach
- Media notification: Breaches affecting more than 500 residents of a state require media notification within 60 days
- HHS Secretary notification: Breaches of 500+ individuals must be reported to HHS OCR within 60 days
- CIRCIA reporting: The Cyber Incident Reporting for Critical Infrastructure Act requires covered entities to report cyber incidents to CISA within 72 hours and ransom payments within 24 hours (final rule expected in 2026)
Organizations that wait until after a breach to identify these obligations routinely miss them - building deadline triggers directly into your IR runbooks eliminates that risk.
Third-Party Vendor Risk
Business Associates represent a disproportionate share of healthcare breach risk. According to Bluesight's 2025 Breach Barometer, Business Associates were involved in 77% of all breached records in 2024, despite representing only 16% of breach reports. That gap means a gap in your IR plan: Business Associate Agreements (BAAs) and vendor-specific response protocols need to be explicit components, not afterthoughts.
Internet of Medical Things (IoMT) and Legacy Devices
Healthcare IR must account for unique infrastructure challenges:
- 53% of all IoT and IoMT devices in hospitals contain vulnerabilities that pose critical risks to patient safety, data confidentiality, or service availability
- 85% of medical organizations use outdated operating systems or infrastructure, such as unsupported Windows XP software
- 20% of healthcare ransomware attacks began with an attack on a medical device
Because these devices often cannot be patched or taken offline without disrupting care, IR teams need pre-approved isolation procedures and compensating controls documented before an incident hits - not improvised during one.
How the Healthcare Incident Response Process Works
Most healthcare IR plans are built on the NIST SP 800-61 (Computer Security Incident Handling Guide) framework, which treats incident response as a continuous lifecycle rather than a one-time checklist. NIST SP 800-61 Revision 3 was published in April 2025 and maps directly to the NIST Cybersecurity Framework (CSF) 2.0 Functions. HHS, OCR, and ASPR TRACIE explicitly reference NIST SP 800-61 as the foundational guideline for healthcare IR.
Preparation
Preparation is the foundation of the entire IR process. This phase involves:
- Building a comprehensive Incident Response Plan (IRP)
- Forming a cross-functional Incident Response Team (IRT) that includes security, legal, compliance, HR, PR, and executive leadership
- Running tabletop exercises and technical restoration drills to ensure every team member knows their role before an incident happens
Organizations that conduct regular tabletop exercises consistently outperform those that rely on documentation alone.
Detection and Analysis
During detection, security teams monitor network traffic, device logs, and alerts using tools like SIEM (Security Information and Event Management) and EDR (Endpoint Detection and Response) to identify potential incidents, filter false positives, and triage confirmed events by severity.
In healthcare, 24/7 monitoring is non-negotiable given the volume of connected devices and the value of PHI to attackers. Cybriant's Managed SIEM provides round-the-clock threat detection for organizations that lack in-house SOC capacity - dedicated security professionals assess alerts in real time and guide remediation.
Containment
Containment follows a two-stage approach:
- Short-term containment: Isolate affected systems to stop the spread (e.g., taking infected devices offline)
- Long-term containment: Apply stronger controls around unaffected systems
Healthcare containment must balance security isolation with maintaining continuity of critical patient care systems. Teams must preserve forensic evidence at this stage rather than wiping it - HIPAA-covered entities must demonstrate exactly what data a threat actor accessed, or they must presume a full breach.
Eradication and Recovery
Eradication means fully removing the threat - malware, unauthorized access, and any backdoors left behind. Recovery follows: restoring affected systems from clean, validated backups, applying patches, and confirming each system is free of compromise before bringing it back online.
Healthcare organizations must validate that PHI integrity has not been compromised before restoring EHR access.
Post-Incident Review
Done well, the post-incident review prevents the same breach from happening twice. This phase includes:
- Root-cause analysis
- Lessons-learned documentation
- Updates to the IRP
- HIPAA breach notification filings if required
- Reporting to HHS OCR or CISA within mandated timeframes
Each review cycle strengthens the next Preparation phase - teams that document specific control gaps close them faster than those that file generic after-action reports.
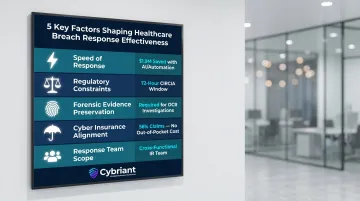
Key Factors That Shape Effective Data Breach Response in Healthcare
Five variables determine whether a healthcare organization contains a breach effectively or spirals into prolonged damage - spanning speed, legal obligations, forensic discipline, financial coverage, and team structure.
Speed of initial response: The first four hours are critical. Organizations using AI and automation in security functions saved $1.9 million compared to those without. Organizations with both an IR team and a tested plan consistently outperform those without.
Regulatory and reporting constraints: HIPAA notification deadlines, CIRCIA's 72-hour reporting window, and state-specific requirements (some states mandate reporting within two hours of discovery) dictate how response must be sequenced and documented from the start.
Forensic evidence preservation: Resist the urge to wipe and rebuild systems quickly. OCR investigations require organizations to demonstrate the exact scope of threat actor access. Sandbox environments preserve forensic integrity while remediation proceeds in parallel.
Cyber insurance alignment: Insurers now require documented proof of implemented controls - MFA, EDR, patch management, offline backups, 24/7 SOC coverage - before paying claims. Review the IR plan and the insurance policy together before an incident. In 2024, 56% of claims reported to Coalition were handled without any out-of-pocket payments by the policyholder.
Scope of the response team: Healthcare organizations that silo IR within IT consistently underperform during breach response. Effective IR requires legal counsel (for privilege protection and OCR navigation), compliance officers (for HIPAA breach assessment), and executive leadership (for business continuity decisions and board-level notification).
Common Misconceptions About Healthcare Incident Response
Having a Documented Plan Equals Being Ready
Plans that sit on shelves and have never been tested through tabletop exercises or technical simulations will fail under real incident conditions. The plan must be a living document exercised regularly against realistic healthcare scenarios - including ransomware, PHI exposure, and medical device compromise.
Paying a Ransom Resolves a Data Breach
Threat actors increasingly use double and triple extortion tactics, contacting patients directly even after a ransom is paid. The FBI and CISA explicitly state that paying a ransom does not guarantee data will be decrypted or that stolen data will be deleted.
Sensitive data should be assumed exfiltrated regardless of payment. That means HIPAA breach notification obligations still apply - and the full IR process must proceed.
Standard Enterprise IR Frameworks Can Be Applied Without Modification
Healthcare adds layers that generic frameworks do not address:
- The PHI breach presumption rule
- BAA-regulated third-party obligations
- IoMT device constraints
- Patient safety considerations that prevent simply taking systems offline during containment without clinical coordination
Healthcare IR plans require custom playbooks that account for these clinical and regulatory constraints from the start - not general-purpose templates retrofitted after the fact.
Conclusion
Healthcare incident response demands more than a generic cybersecurity playbook. Patient safety, HIPAA obligations, evidence preservation, and cross-functional coordination all shape how a breach unfolds - and how quickly an organization recovers.
The difference between organizations that recover quickly and those that suffer prolonged disruption and regulatory action is consistently preparation. Organizations that invest in 24/7 monitoring, automated threat detection, and formal IR planning before an incident occurs are far better positioned to contain damage, meet regulatory deadlines, and keep patient care running. The plan sitting untested on a shelf won't save you - the one your team has drilled will.
Cybriant's 24/7 Managed SIEM and around-the-clock threat detection give healthcare organizations the monitoring and response capability that effective incident response depends on - without building an internal SOC. Call 844-411-0404 to discuss strengthening your incident response readiness.
Frequently Asked Questions
What is the incident response team process?
The incident response team process follows a structured lifecycle: Preparation, Detection and Analysis, Containment, Eradication, Recovery, and Post-Incident Review. The team activates specific roles and documented procedures at each phase to limit damage and restore operations.
Who is the incident response team?
The incident response team (IRT or CSIRT) in healthcare is a cross-functional group that typically includes the security officer, privacy officer, legal counsel, compliance, HR, executive leadership, IT, and may also involve external forensic or MSSP partners.
What are P1, P2, P3, and P4 incidents?
P1–P4 are incident priority classifications used to triage severity: P1 (critical) requires immediate all-hands response, P2 (high) needs urgent attention, P3 (medium) is addressed within normal workflows, and P4 (low) is logged and monitored. In healthcare, any incident involving PHI is typically treated as at minimum P2.
What are the 7 components of incident response?
While NIST defines 4 main phases, expanded frameworks often cite 7 components: Preparation, Detection, Triage, Analysis, Containment, Eradication, and Recovery. Post-Incident Review is sometimes added as an eighth - and in healthcare, HIPAA breach assessment must be integrated into the analysis stage.
What are the 5 components of ICS?
ICS (Incident Command System) includes five components: Command, Operations, Planning, Logistics, and Finance/Administration. Originally a disaster management framework, ICS is now applied to large-scale cybersecurity incidents in healthcare where multiple departments and external agencies must be coordinated.
What are the 5 C's of incident management?
The 5 C's of incident management are: Confirm (verify an incident has occurred), Contain (limit the spread), Control (stabilize the environment), Communicate (notify stakeholders and regulators), and Close (remediate and conduct post-incident review). In healthcare, Communicate carries additional weight due to HIPAA's mandatory notification timelines.


